What is OCD?
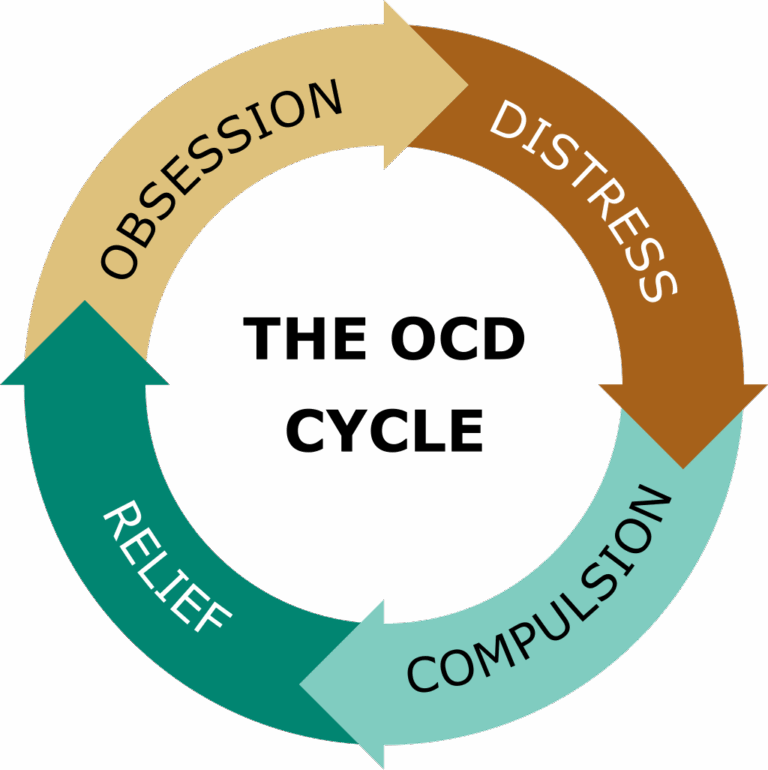
There is a widespread misconception that obsessive-compulsive disorder (OCD) is simply a personality quirk or a preference for neatness, often leading people to say they’re “a little bit OCD.” In truth, OCD is a serious and often debilitating mental health condition that can affect individuals of all ages and backgrounds. It is characterized by a persistent cycle of obsessions and compulsions.
Obsessions are unwanted, intrusive thoughts, images, or urges that cause intense anxiety or distress. In response, individuals engage in compulsions—repetitive behaviors or mental acts—intended to reduce the distress or prevent a feared outcome.
While many people may occasionally experience obsessive thoughts or compulsive behaviors, this does not mean they have OCD. For an OCD diagnosis, the cycle of obsessions and compulsions must be severe enough to consume significant time (typically more than an hour per day), cause substantial distress, or interfere with daily functioning and important life activities.
Types of OCD
Harm OCD
Harm OCD is a subtype of Obsessive-Compulsive Disorder in which a person experiences intense fear or distress about causing harm to themselves or others—either accidentally or on purpose. These fears are unwanted and go against the individual’s values, making them deeply distressing.
Key Features of Harm OCD:
Obsessions:
These are unwanted, intrusive thoughts, images, or urges related to harming others or oneself. Common examples include:
“What if I snap and hurt someone I love?”
“What if I lose control and stab myself with this knife?”
“What if I ran someone over and didn’t notice?”
“What if I’m secretly a violent person?”
Compulsions:
To relieve the anxiety caused by these obsessions, individuals may engage in compulsive behaviors. These can include:
Avoiding knives, driving, or being alone with loved ones
Repeatedly checking to make sure they haven’t harmed anyone
Mentally reviewing past actions for reassurance
Seeking constant reassurance from others (“I’d never hurt anyone, right?”)
Repeating prayers or phrases to neutralize the thought
Impact on Daily Life:
Harm OCD can significantly interfere with a person’s ability to function. Everyday activities like cooking, spending time with children, or even driving can become sources of extreme fear and avoidance. These behaviors are not signs of actual violent intent—they are driven by overwhelming anxiety and a deep desire not to cause harm.
It’s Important to Note:
People with Harm OCD are not dangerous. In fact, they are usually highly empathetic and distressed by their thoughts.
The intrusive thoughts are ego-dystonic—meaning they go against the person’s true character and values.
Harm OCD is often misunderstood, even by clinicians, which makes proper diagnosis and treatment essential.
Counting OCD
Counting OCD is a subtype of Obsessive-Compulsive Disorder in which a person feels a strong urge to count or perform actions a specific number of times to prevent something bad from happening or to make things feel “just right.” These counting rituals are driven by anxiety and are not simply habits—they are compulsive behaviors aimed at reducing distress from intrusive thoughts or sensations.
Key Features of Counting OCD:
Obsessions:
These are unwanted, intrusive thoughts or urges that create a sense of anxiety or incompleteness unless a specific counting ritual is performed. Common examples include:
“If I don’t count to 8, my family will get hurt.”
“I have to step in even numbers or something bad will happen.”
“If I don’t tap this 4 times, I’ll fail at my job.”
“I lost track of my counting—now I have to start over.”
Compulsions:
To relieve the anxiety caused by these obsessions, individuals may engage in repetitive counting behaviors, such as:
Counting in specific patterns (e.g., by 2s, 3s, 5s)
Repeating actions a certain number of times (e.g., flicking a light switch 6 times)
Avoiding “unlucky” numbers or favoring “safe” or “special” numbers
Mentally counting while walking, talking, or doing tasks
Restarting actions if the “right” number wasn’t reached
Impact on Daily Life:
Counting OCD can make even simple tasks feel overwhelming and time-consuming. Walking, eating, getting dressed, or interacting with others may be delayed or disrupted by the need to count or repeat actions. These rituals can interfere with work, school, relationships, and daily functioning.
It’s Important to Note:
People with Counting OCD usually know the counting isn’t logical, but feel immense anxiety if they resist it.
The counting is not about superstition—it’s about trying to neutralize fear, discomfort, or a sense of impending doom.
The “right” number often varies by person and may be tied to personal meaning, symmetry, or simply what feels safe.
Hoarding OCD
Hoarding OCD is a subtype of Obsessive-Compulsive Disorder in which a person experiences intense anxiety about discarding or parting with possessions, regardless of their actual value. This fear is typically driven by obsessive thoughts and is followed by compulsive behaviors related to acquiring or saving items.
Key Features of Hoarding OCD:
Obsessions:
These are intrusive, distressing thoughts or fears related to losing items or needing to keep them. Common obsessions include:
“What if I need this someday?”
“If I throw this away, something bad might happen.”
“This item might be important, even if it looks useless.”
Compulsions:
In response to these obsessive thoughts, individuals may:
Save or collect seemingly unnecessary items (e.g., newspapers, old clothes, broken appliances)
Avoid throwing things away, even trash or expired items
Repeatedly check stored items to make sure they’re still there
Feel compelled to organize or rearrange belongings, often without making progress
Impact on Daily Life:
Hoarding OCD can severely disrupt daily functioning. Living spaces may become cluttered and unusable, creating health and safety hazards. Relationships with family and friends can suffer due to the clutter or secrecy about hoarding behaviors. The emotional distress is often profound, including guilt, shame, and social isolation.
"Just Right" OCD
Order & Symmetry OCD is a subtype of Obsessive-Compulsive Disorder in which a person experiences intense discomfort, distress, or anxiety when things feel “off,” misaligned, or not arranged in a “just right” way. The need for order or symmetry is often driven by a deep internal sense that something is wrong, incomplete, or unsafe unless corrected.
Key Features of Order & Symmetry OCD:
Obsessions:
These are unwanted, intrusive thoughts or sensations related to things being uneven, out of place, or not feeling “right.” Common examples include:
“This picture frame isn’t perfectly straight—it’s bothering me.”
“These books aren’t arranged symmetrically, and it feels wrong.”
“My body doesn’t feel balanced unless I tap the other side.”
“If I don’t fix this, something bad might happen.”
Compulsions:
To relieve the distress caused by these obsessions, individuals may engage in compulsive behaviors aimed at achieving perfect order, symmetry, or balance. These can include:
Rearranging objects until they are “just right”
Lining up items symmetrically or by size/color
Rewriting, retyping, or redrawing repeatedly
Tapping or touching things a certain number of times or equally on both sides of the body
Avoiding environments where order or symmetry can’t be maintained
Impact on Daily Life:
Order & Symmetry OCD can make everyday environments feel overwhelming or intolerable. Tasks like organizing a desk, folding laundry, or even walking through a room can become exhausting rituals. The distress is not about aesthetics or perfectionism—it’s driven by anxiety, discomfort, or an overwhelming fear that something bad will happen if things aren’t aligned “just right.”
It’s Important to Note:
People with this subtype often know their need for symmetry or order is excessive, but they feel powerless to stop the compulsions.
This isn’t about being neat or tidy for appearance’s sake—it’s about reducing mental discomfort or avoiding perceived danger.
For some, the compulsion is not connected to a fear of harm but rather a need to neutralize the unbearable sense that something is “off.”
Relationship OCD
Relationship OCD (ROCD) is a subtype of Obsessive-Compulsive Disorder in which a person experiences intrusive doubts, fears, or preoccupations about their romantic relationship. These thoughts can center around whether they truly love their partner, whether their partner loves them, or whether the relationship is “right.” The doubts are persistent and distressing, even if the relationship is healthy and supportive.
Key Features of Relationship OCD:
Obsessions:
These are unwanted, intrusive thoughts, questions, or feelings about the relationship or partner. Common examples include:
“What if I don’t really love my partner?”
“What if I’m settling and there’s someone better out there?”
“What if they’re not ‘the one’?”
“What if my lack of excitement today means I’m with the wrong person?”
“Do they love me enough?”
Compulsions:
To relieve the anxiety caused by these obsessions, individuals may engage in compulsive behaviors such as:
Constantly analyzing the relationship for flaws or reassurance
Comparing their partner or relationship to others’
Seeking reassurance from friends, family, or their partner (“Do you think we’re right for each other?”)
Mentally reviewing past moments to confirm or deny feelings
Testing their feelings by imagining breakups or other partners
Impact on Daily Life:
Relationship OCD can deeply strain a person’s connection with their partner. The constant questioning and need for certainty can make it hard to be present or enjoy the relationship. Even in a stable, loving relationship, the individual may feel stuck in doubt, guilt, or fear—leading to emotional distance or repeated breakups and reconciliations.
It’s Important to Note:
ROCD is not the same as healthy relationship concerns—it involves obsessive doubt and compulsive mental or behavioral rituals to gain certainty.
People with ROCD often deeply value their partner but feel tortured by the inability to feel sure enough.
The goal of treatment is not to answer the question “Is this the right person?” but to help the individual tolerate uncertainty and stop compulsive behaviors.
Existential OCD
Existential OCD is a subtype of Obsessive-Compulsive Disorder in which a person becomes consumed by intrusive, distressing thoughts or questions about the nature of existence, reality, the self, or the universe. These deep, philosophical questions are not just curiosities—they cause overwhelming anxiety and can feel impossible to “turn off.”
Key Features of Existential OCD:
Obsessions:
These are unwanted, intrusive thoughts or questions about life, reality, identity, or meaning. Common examples include:
“What if none of this is real?”
“How do I know I even exist?”
“What if life has no meaning and never will?”
“What if I’m stuck in a simulation?”
“What is the point of anything if we all die anyway?”
Compulsions:
To relieve the anxiety caused by these obsessions, individuals may engage in mental or behavioral rituals. These can include:
Constantly analyzing or ruminating on existential questions
Researching philosophy, science, or religion in search of certainty
Asking others for reassurance (“Do you ever think about this too?”)
Avoiding certain topics, media, or situations that trigger existential thoughts
Repeating comforting phrases or mental “solutions” to reduce anxiety
Impact on Daily Life:
Existential OCD can make it difficult to engage with the world in a grounded or present way. Activities like watching movies, reading, or even having conversations can trigger overwhelming spirals of doubt and fear. The person may feel detached from themselves or reality, struggling to find meaning or connection, even when life appears fine from the outside.
It’s Important to Note:
Existential questions are normal—but in Existential OCD, they become obsessive, distressing, and impair functioning.
The goal of treatment is not to find definitive answers to life’s biggest questions, but to help individuals sit with uncertainty and reduce compulsive searching or rumination.
This subtype can often be confused with depression or philosophical pondering, but in OCD, the key difference is the anxiety and compulsions that follow.
Pedophilia OCD
Pedophilia OCD (POCD) is a subtype of Obsessive-Compulsive Disorder in which a person experiences intrusive, unwanted thoughts, images, or fears about being sexually attracted to children. These thoughts are deeply distressing, go against the person’s values, and are not reflective of their desires or intentions.
Key Features of Pedophilia OCD:
Obsessions:
These are unwanted, intrusive thoughts or fears about harming a child or being attracted to them. Common examples include:
“What if I’m secretly a pedophile?”
“Why did I feel something when I saw that child?”
“What if I touched that child inappropriately without knowing?”
“What if I lose control and hurt a kid?”
Compulsions:
To relieve the anxiety caused by these obsessions, individuals may engage in compulsive mental or behavioral rituals. These can include:
Avoiding children or places where children may be present
Mentally reviewing interactions to check for inappropriate behavior
Repeatedly seeking reassurance from others (“You don’t think I’m a bad person, right?”)
Researching signs of pedophilia to “prove” they don’t fit the criteria
Testing their reactions to children to “make sure” they’re not attracted
Impact on Daily Life:
POCD can lead to intense shame, guilt, and isolation. People with this subtype often go to great lengths to avoid any situation involving children—even if they previously enjoyed time with family or had a career in childcare. The fear of “what if” can become all-consuming, even when the person has never acted on or desired to act on such thoughts.
It’s Important to Note:
POCD is not the same as pedophilia. People with POCD are repulsed and terrified by their thoughts, not aroused by them.
The thoughts are ego-dystonic, meaning they go against the person’s identity, values, and desires.
The distress comes from the fear of what the thoughts mean, not from a desire to act on them.
Treatment:
Exposure and Response Prevention (ERP) is the gold-standard therapy, helping individuals face the thoughts without engaging in reassurance or avoidance.
Cognitive-behavioral therapy (CBT) and sometimes SSRIs may also be helpful.
Because of stigma and fear of being misunderstood, many people with POCD suffer in silence—finding an OCD-specialized therapist is crucial.
Contamination OCD
Contamination OCD is a subtype of Obsessive-Compulsive Disorder in which a person experiences intense fear or distress about being contaminated by germs, dirt, chemicals, or other perceived impurities. This fear can also extend to contaminating others or their environment.
Key Features of Contamination OCD:
Obsessions:
These are unwanted, intrusive thoughts, images, or urges related to contamination. Common examples include:
“What if I get sick from touching this doorknob?”
“What if I spread germs to my family?”
“This item feels dirty, even though I just cleaned it.”
Compulsions:
To relieve the anxiety caused by these obsessions, individuals may engage in compulsive behaviors. These can include:
Excessive hand washing or showering
Avoiding touching certain objects or surfaces
Cleaning or disinfecting items repeatedly
Changing clothes frequently
Avoiding public spaces or people they fear may be “contaminated”
Impact on Daily Life:
Contamination OCD can significantly interfere with a person’s ability to function. Routine activities like using public transportation, grocery shopping, or even hugging loved ones can become overwhelming or impossible. These behaviors are not just preferences for cleanliness—they are driven by intense fear and anxiety.
It’s Important to Note:
People with Contamination OCD often recognize that their fears may be irrational, but they feel powerless to stop the obsessions and compulsions.
This subtype became especially prominent during events like the COVID-19 pandemic, where public health concerns blurred the line between appropriate caution and OCD-driven behavior.
Religious OCD
Religious OCD (Scrupulosity) is a subtype of Obsessive-Compulsive Disorder in which a person experiences intense fear or distress about being morally or spiritually impure, sinful, or offensive to a higher power. These fears are driven by unwanted thoughts, not a lack of faith, and often lead to compulsive behaviors aimed at achieving moral or religious “perfection.”
Key Features of Religious OCD:
Obsessions:
These are unwanted, intrusive thoughts, doubts, or images related to religion, morality, or offending a higher power. Common examples include:
“What if I accidentally blasphemed?”
“What if God is angry with me?”
“What if I didn’t pray the right way and now I’ll be punished?”
“What if that thought I just had was sinful?”
“What if I’m not really faithful enough and I go to hell?”
Compulsions:
To relieve the anxiety caused by these obsessions, individuals may engage in mental or physical rituals such as:
Excessive praying or repeating religious phrases until it feels “just right”
Seeking reassurance from religious leaders or loved ones about moral purity
Avoiding people, places, or objects that might trigger “impure” thoughts
Re-reading sacred texts or redoing religious rituals repeatedly
Mentally reviewing past actions or thoughts to ensure they were not sinful
Impact on Daily Life:
Religious OCD can interfere with a person’s ability to practice their faith in a peaceful, meaningful way. What might be a source of comfort for others becomes a source of fear, guilt, and distress. It can also lead to isolation, constant doubt, and feelings of unworthiness, despite the person’s deep commitment to their beliefs.
It’s Important to Note:
Religious OCD is not a lack of faith—it often occurs in people who care deeply about their values and beliefs.
The thoughts are ego-dystonic, meaning they are unwanted and go against the person’s true intentions or desires.
Religious or moral themes are being hijacked by OCD—not chosen by the individual.
Treatment:
Exposure and Response Prevention (ERP) is highly effective, helping individuals confront the fear of imperfection while resisting compulsive rituals.
Faith leaders who understand OCD can be supportive allies, especially when treatment is integrated respectfully with religious values.
Working with an OCD-informed therapist is key—this subtype is often misunderstood or misdiagnosed.
False Memory OCD
False Memory OCD is a subtype of Obsessive-Compulsive Disorder in which a person becomes fixated on intrusive doubts about past events—often fearing they did or said something wrong, immoral, or harmful, even if there’s little or no evidence that it happened. These thoughts often feel vivid and convincing, leading to overwhelming guilt and a desperate need for certainty.
Key Features of False Memory OCD:
Obsessions:
These are unwanted, intrusive doubts or mental images about past experiences. The thoughts often question the accuracy of one’s memory or create false narratives. Common examples include:
“What if I said something offensive and don’t remember it?”
“What if I cheated on my partner and blocked it out?”
“What if I hit someone with my car and didn’t realize it?”
“What if I committed a crime years ago and forgot?”
Compulsions:
To relieve the anxiety caused by these obsessions, individuals may engage in mental or behavioral rituals, such as:
Repeatedly mentally reviewing the past to try to “prove” what happened
Seeking reassurance from others about their behavior or character
Avoiding certain people, places, or situations connected to the memory
Googling symptoms or stories to compare experiences
Confessing thoughts or imagined actions to others
Impact on Daily Life:
False Memory OCD can lead to extreme distress, guilt, and self-doubt. Even minor or entirely imagined incidents can become the focus of obsessive rumination for days, weeks, or even years. Relationships may suffer due to constant confessing or avoidance, and work or social functioning can be disrupted by persistent mental checking and anxiety.
It’s Important to Note:
These memories feel real, but that does not make them true.
People with False Memory OCD are usually highly moral and sensitive individuals who would be devastated by doing harm—yet that fear is exactly what OCD latches onto.
The goal of treatment is not to find certainty, but to accept uncertainty and break the cycle of obsession and compulsion.
Magical Thinking OCD
Magical Thinking OCD is a subtype of Obsessive-Compulsive Disorder in which a person believes that their thoughts, actions, or words—though logically unrelated—can somehow influence or prevent unrelated events from happening. These beliefs are not rooted in reality, but the person feels intense anxiety or fear that something bad will happen if they don’t follow certain rituals or thought patterns.
Key Features of Magical Thinking OCD:
Obsessions:
These are unwanted, intrusive thoughts or beliefs that link unrelated events or ideas. The person fears that not following certain mental rules could lead to harm or disaster. Common examples include:
“If I think about someone dying, it might make it happen.”
“If I don’t say this phrase in my head, my mom will get in a car crash.”
“If I step on a crack, something bad will happen to my family.”
“If I don’t avoid this number, I’ll fail my exam.”
Compulsions:
To relieve the anxiety caused by these obsessions, individuals may engage in compulsive behaviors or mental rituals. These can include:
Repeating specific words, phrases, or prayers “just right”
Avoiding “bad” numbers, words, or colors
Performing rituals like tapping, blinking, or touching objects a certain way
Mentally canceling out “bad” thoughts with “good” ones
Avoiding situations that might trigger intrusive magical thoughts
Impact on Daily Life:
Magical Thinking OCD can significantly interfere with day-to-day functioning. Tasks may take much longer due to ritualistic behaviors, and the person may avoid activities, people, or places out of fear that something terrible will happen if they don’t obey their mental rules. The compulsions can become exhausting and isolating.
It’s Important to Note:
People with Magical Thinking OCD often recognize that their beliefs are irrational or exaggerated, but the fear of being responsible for harm feels too overwhelming to ignore.
This subtype often targets people who feel deeply responsible for others and fear being the cause of harm, even in far-fetched ways.
The “magic” isn’t real—it’s OCD’s way of tricking the brain into thinking safety depends on performing rituals or avoiding triggers.
Perinatal & Postpartum OCD
Perinatal and Postpartum OCD is a subtype of Obsessive-Compulsive Disorder that occurs during pregnancy (perinatal) or after childbirth (postpartum). It is marked by unwanted, intrusive thoughts related to the baby’s safety, the parent’s competency, or fears of causing harm—often paired with compulsive behaviors or mental rituals aimed at reducing this intense anxiety.
Key Features of Perinatal/Postpartum OCD:
Obsessions:
These are intrusive, distressing thoughts, images, or urges that revolve around the baby or parenting. Common examples include:
“What if I accidentally drop my baby?”
“What if I snap and hurt my baby on purpose?”
“What if I made a mistake feeding or changing them and didn’t realize it?”
“What if I’m not bonding the way I should—does that mean I’m a bad mother?”
“What if I’m not meant to be a parent?”
Compulsions:
To reduce the fear or guilt caused by these thoughts, individuals may engage in rituals or avoidance behaviors such as:
Excessively checking on the baby’s breathing or safety
Avoiding being alone with the baby out of fear they may cause harm
Repeatedly researching parenting topics to ensure they’re doing everything “right”
Seeking constant reassurance from partners, doctors, or family
Mentally reviewing past actions for signs of wrongdoing
Impact on Daily Life:
Perinatal and Postpartum OCD can be overwhelming during a time when parents are already vulnerable and exhausted. The thoughts often clash with a parent’s deep love and commitment, which makes them especially distressing. This subtype can interfere with bonding, cause intense shame or guilt, and lead to isolation or depression if not treated.
It’s Important to Note:
Intrusive thoughts of harm do not mean someone wants to hurt their baby. In fact, they’re usually a sign of how much they care.
These thoughts are ego-dystonic, meaning they go against the person’s core values and are unwanted and terrifying.
Perinatal OCD is different from postpartum psychosis. In OCD, the person has insight, is horrified by the thoughts, and does not act on them.
Checking OCD
Checking OCD is a subtype of Obsessive-Compulsive Disorder in which a person experiences intense fear or anxiety that something bad will happen if they don’t repeatedly check certain things. This fear can involve harm coming to oneself or others due to negligence, forgetfulness, or making a mistake.
Key Features of Checking OCD:
Obsessions:
These are unwanted, intrusive thoughts, images, or urges related to making a mistake or causing harm through inattention or carelessness. Common examples include:
“What if I left the stove on and the house burns down?”
“What if I didn’t lock the door and someone breaks in?”
“What if I ran someone over without realizing it?”
“What if I made a typo in that important email and get fired?”
Compulsions:
To relieve the anxiety caused by these obsessions, individuals may engage in compulsive checking behaviors. These can include:
Repeatedly checking appliances (e.g., stove, iron, hair straightener)
Rechecking locks, doors, and windows
Going back to retrace driving routes to make sure no one was harmed
Rereading messages or emails dozens of times before sending them
Seeking reassurance from others (“Are you sure I turned it off?”)
Impact on Daily Life:
Checking OCD can significantly interfere with a person’s ability to complete daily tasks or leave the house. What might take someone else seconds—like locking a door—can take someone with Checking OCD several minutes or even hours due to repeated checks. These behaviors are not habits—they are driven by intense fear, guilt, and doubt.
It’s Important to Note:
People with Checking OCD are not careless—they are often overly conscientious and fearful of being responsible for harm.
The fear of uncertainty (“What if I missed something?”) is a driving force behind checking compulsions.
Checking may provide temporary relief, but it reinforces the obsession and increases anxiety over time.
Sexual Orientation OCD
Sexual Orientation OCD (SO-OCD) is a subtype of Obsessive-Compulsive Disorder in which a person experiences intrusive, distressing thoughts, doubts, or mental images about their sexual orientation. These thoughts are not reflective of actual desires but trigger intense anxiety, guilt, and confusion, leading to compulsive behaviors to seek certainty.
Key Features of Sexual Orientation OCD:
Obsessions:
These are unwanted, intrusive thoughts or fears about possibly being a different sexual orientation than one identifies with. Common examples include:
“What if I’m actually gay/straight and don’t know it?”
“What if I’ve been lying to myself this whole time?”
“Why did I notice that person—does that mean I’m attracted to them?”
“What if I’m living a lie and hurting my partner?”
“What if a single thought or feeling proves I’m not who I say I am?”
Compulsions:
To reduce the anxiety caused by these obsessions, individuals may engage in repetitive mental or behavioral rituals such as:
Mentally analyzing or reviewing one’s past relationships or attractions
Watching adult content to “test” reactions
Avoiding certain people, situations, or media out of fear they’ll feel something
Seeking reassurance from others (“Do I seem gay/straight/bi to you?”)
Repeating affirmations or checking feelings to try to feel “100% sure”
Impact on Daily Life:
SO-OCD can be deeply distressing, especially in cultures or communities where identity and orientation are strongly tied to personal or religious values. The obsession is not about actual exploration or identity questioning—it’s about needing certainty and trying to eliminate doubt. The thoughts are experienced as intrusive and unwanted, and the compulsive checking can consume hours of mental space and energy each day.
It’s Important to Note:
SO-OCD is not the same as being closeted or questioning—it involves intrusive thoughts that go against the person’s sense of self and cause significant anxiety.
These thoughts are ego-dystonic, meaning they are unwanted and inconsistent with the person’s values and identity.
Many people with SO-OCD fear that having the thoughts “must mean something,” but in reality, thoughts are not facts.
Suicidal OCD
Suicidal OCD is a subtype of Obsessive-Compulsive Disorder in which a person experiences intrusive, unwanted thoughts or fears about ending their own life—despite not wanting to die. These thoughts are not expressions of intent, but rather cause extreme anxiety, confusion, and guilt. The person fears they might lose control and act on the thoughts, even though they have no desire to do so.
Key Features of Suicidal OCD:
Obsessions:
These are unwanted, intrusive thoughts, images, or urges related to suicide. Common examples include:
“What if I suddenly lose control and kill myself?”
“What if I secretly want to die and don’t know it?”
“What if I’m holding a knife and suddenly use it on myself?”
“What if I jump off that balcony, even though I don’t want to?”
“Does having this thought mean I’m depressed or dangerous?”
Compulsions:
To relieve the intense fear and anxiety caused by these obsessions, individuals may engage in compulsive behaviors or mental rituals, such as:
Avoiding sharp objects, high places, or medications
Constantly seeking reassurance from others or online (e.g., “Does this mean I’m suicidal?”)
Mentally reviewing thoughts to “prove” they are not suicidal
Monitoring feelings constantly to check for hidden suicidal intent
Repeating phrases or prayers to “cancel out” the thoughts
Impact on Daily Life:
Suicidal OCD can cause extreme emotional distress, fear of being misunderstood, and isolation. Many people avoid seeking help due to fear that others will misinterpret their thoughts as suicidal intent. The condition can interfere with daily activities, relationships, and even a person’s ability to trust their own mind.
It’s Important to Note:
Suicidal OCD is not the same as being suicidal. People with this subtype do not want to die—in fact, they are typically terrified by the idea.
The thoughts are ego-dystonic, meaning they go against the person’s true desires, values, and intentions.
These obsessions stem from anxiety and OCD, not from a genuine wish to harm oneself.